

ICD-10-CM Coding for Hemorrhoids Simplified – Medical Coding Buff Expand Search Toggle Menu Search Previous Continue Search Expand Toggle Menu Close Search
Learn the different types of hemorrhoids, symptoms, causes, complications, diagnosis, and ICD-10-CM coding for hemorrhoids. Coding examples are provided. Medical Coding Buff
ICD-10-CM Coding for Hemorrhoids Simplified – Medical Coding Buff Expand Search Toggle Menu Search Previous Continue Search Expand Toggle Menu Close Search
Learn the different types of hemorrhoids, symptoms, causes, complications, diagnosis, and ICD-10-CM coding for hemorrhoids. Coding examples are provided. Medical Coding Buff
AMA Confirms Proper Coding for Ultroid Hemorrhoid Treatment – AAPC Knowledge Center
Until recently, providers using Ultroid® didn’t have a clear code choice to report Ultroid® treatment as a nonsurgical method to treat hemorrhoids.
ICD-10-CM Coding for Hemorrhoids Simplified – Medical Coding Buff Expand Search Toggle Menu Search Previous Continue Search Expand Toggle Menu Close Search
Learn the different types of hemorrhoids, symptoms, causes, complications, diagnosis, and ICD-10-CM coding for hemorrhoids. Coding examples are provided. Medical Coding Buff
ICD-10-CM Coding for Hemorrhoids Simplified – Medical Coding Buff Expand Search Toggle Menu Search Previous Continue Search Expand Toggle Menu Close Search
Learn the different types of hemorrhoids, symptoms, causes, complications, diagnosis, and ICD-10-CM coding for hemorrhoids. Coding examples are provided. Medical Coding Buff
hemorrhoid – Wikidata
vascular structures in the anal canal
ICD-10-CM Coding for Hemorrhoids Simplified – Medical Coding Buff Expand Search Toggle Menu Search Previous Continue Search Expand Toggle Menu Close Search
Learn the different types of hemorrhoids, symptoms, causes, complications, diagnosis, and ICD-10-CM coding for hemorrhoids. Coding examples are provided. Medical Coding Buff

Hemorrhoids Or Cancer – How To Spot The Difference
Hemorrhoids and cancer have some overlapping symptoms, which can make it difficult to determine if hemorrhoids or cancer is at the root of your issue.
Hemorrhoids

Hemorrhoidectomy CPT code – simplify medical coding – YouTube
Simplify Medical coding Institute. Online Courses offered. Basic and Advanced Medical coding. CPC Exam training. Whatsapp: +91 9360951544.simplify medical…

List of drugs/medicine used for Hemorrhoids (Piles)
View list of generic and brand names of drugs used for treatment of Hemorrhoids(Piles ). Find more information including dose, side effects of the Hemorrhoids(Piles ).
Hemorrhoids: Diagnosis and Treatment Options | AAFP
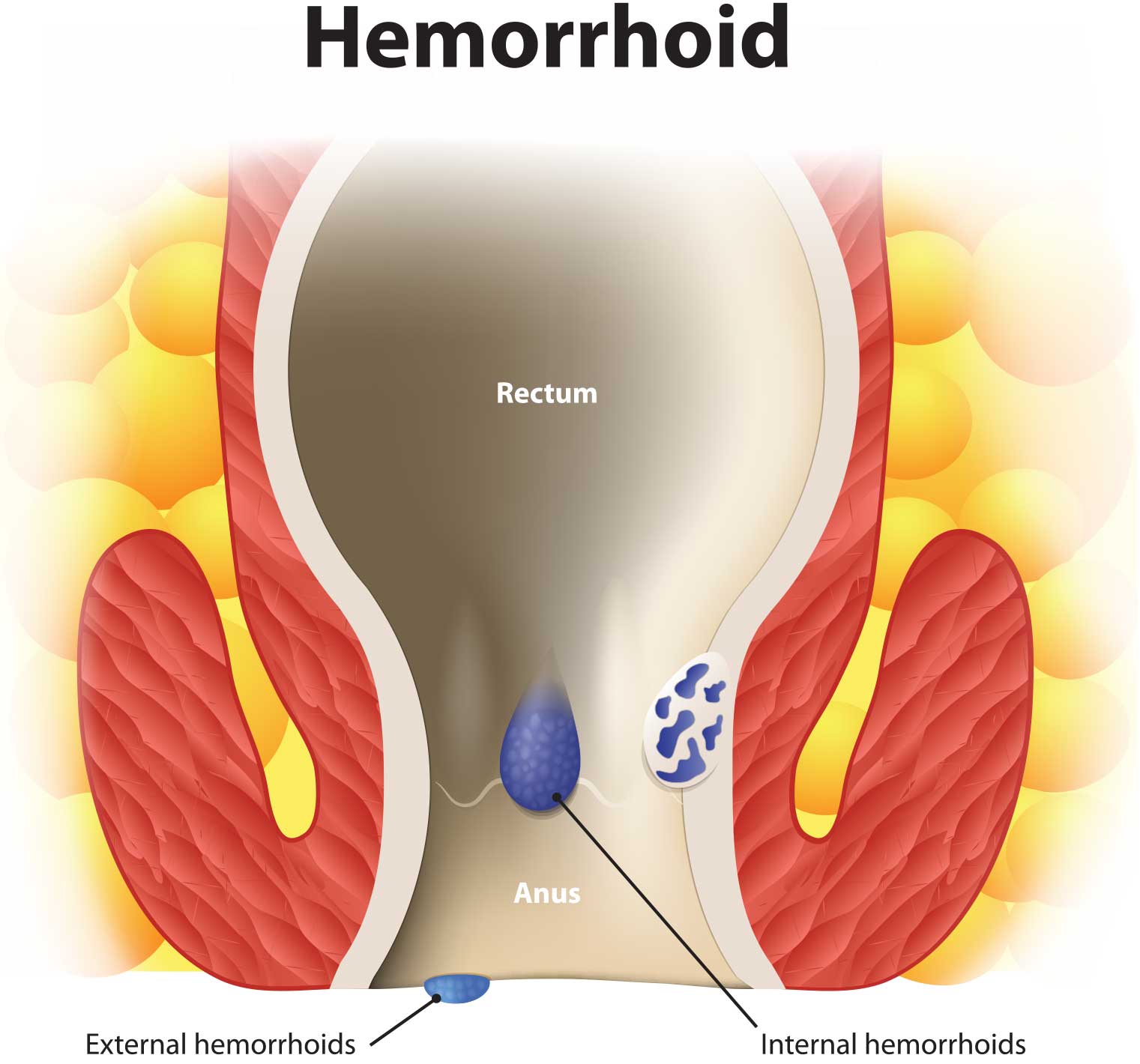
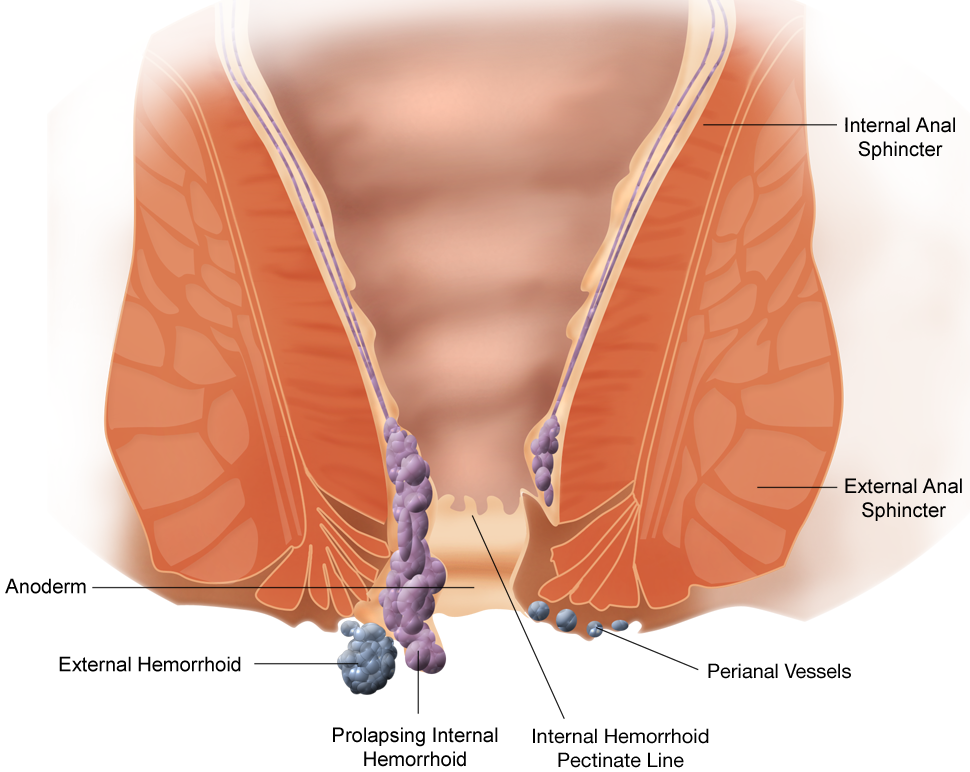
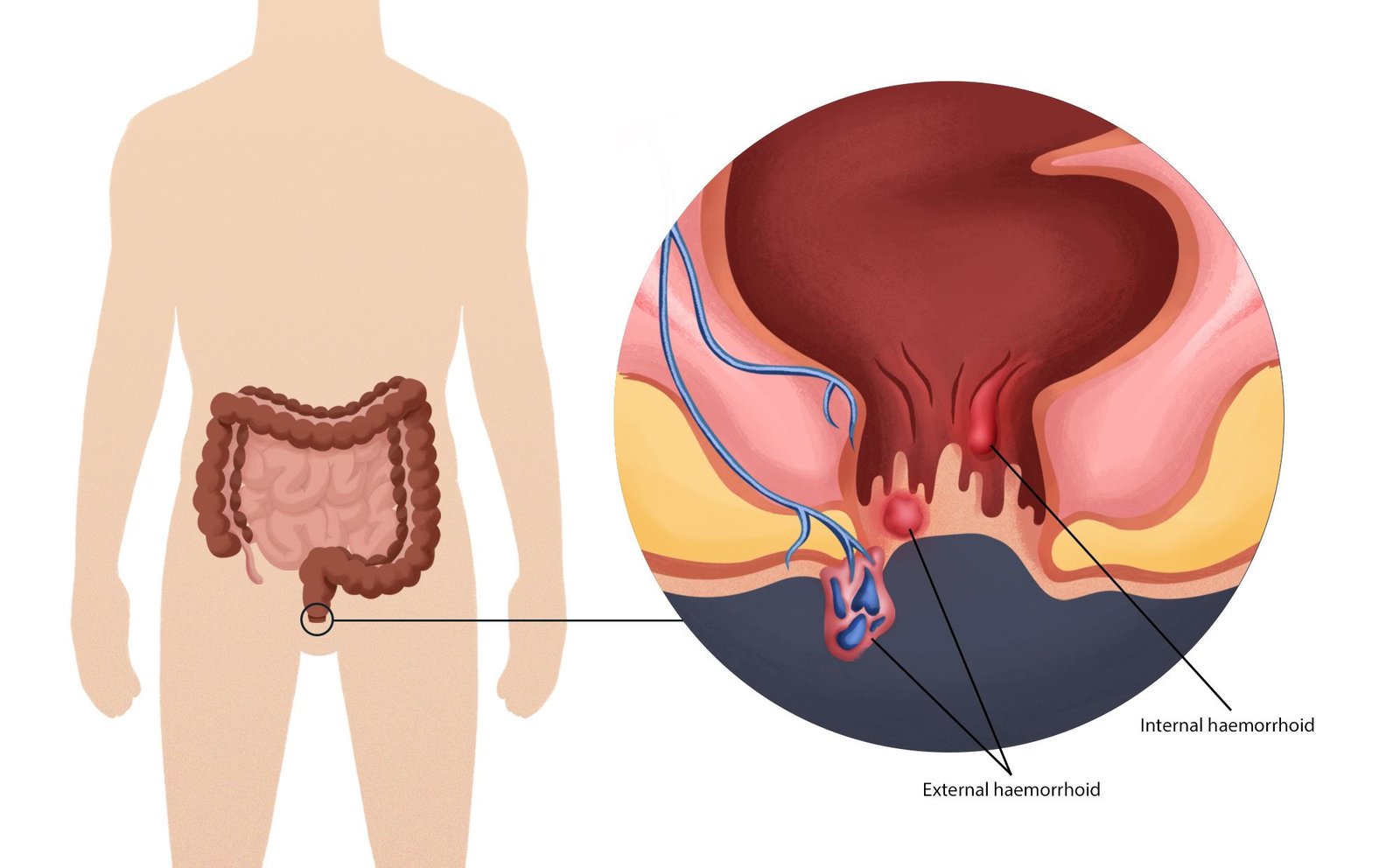
Many Americans between 45 and 65 years of age experience hemorrhoids. Hemorrhoidal size, thrombosis, and location (i.e., proximal or distal to the dentate line) determine the extent of pain or discomfort. The history and physical examination must assess for risk factors and clinical signs indicating more concerning disease processes. Internal hemorrhoids are traditionally graded from I to IV based on the extent of prolapse. Other factors such as degree of discomfort, bleeding, comorbidities, and patient preference should help determine the order in which treatments are pursued. Medical management (e.g., stool softeners, topical over-the-counter preparations, topical nitroglycerine), dietary modifications (e.g., increased fiber and water intake), and behavioral therapies (sitz baths) are the mainstays of initial therapy. If these are unsuccessful, office-based treatment of grades I to III internal hemorrhoids with rubber band ligation is the preferred next step because it has a lower failure rate than infrared photocoagulation. Open or closed (conventional) excisional hemorrhoidectomy leads to greater surgical success rates but also incurs more pain and a prolonged recovery than office-based procedures; therefore, hemorrhoidectomy should be reserved for recurrent or higher-grade disease. Closed hemorrhoidectomy with diathermic or ultrasonic cutting devices may decrease bleeding and pain. Stapled hemorrhoidopexy elevates grade III or IV hemorrhoids to their normal anatomic position by removing a band of proximal mucosal tissue; however, this procedure has several potential postoperative complications. Hemorrhoidal artery ligation may be useful in grade II or III hemorrhoids because patients may experience less pain and recover more quickly. Excision of thrombosed external hemorrhoids can greatly reduce pain if performed within the first two to three days of symptoms.

Stapled hemorrhoidopexy – Wikipedia
Hemorrhoids Or Cancer – How To Spot The Difference
Hemorrhoids and cancer have some overlapping symptoms, which can make it difficult to determine if hemorrhoids or cancer is at the root of your issue.
Diagnosa Ambeien, Ini Kode Yang Perlu Anda Ketahui – Vena Wasir
K.64 adalah kode diagnosa ambeien yang digunakan dalam rekam medis BPJS Kesehatan. Diagnosa ambeien dilakukan melalui pemeriksaan fisik
Hemorrhoid self removal
What Happens When You Squeeze or Pop ItWe include products we think are useful for our readers. If you buy through links on this page, we may earn a small commission. Here’s our process. Can you pop a…
ICD-10 Version:2010
ICD-10 Online contains the ICD-10 (International Classification of Diseases 10th Revision)
Digestive Health Associates
Review of frequently asked questions relating to colonoscopy

IJERPH | Free Full-Text | Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study
Colorectal cancer (CRC) is a common disease and one of the leading causes of cancer deaths worldwide. This retrospective cohort study evaluated the risk of developing CRC in people with hemorrhoids. Using Taiwan’s National Health Insurance Research Database, we established three sets of retrospective study cohorts with and without hemorrhoids. The first set of cohorts were matched by sex and age, the second set of cohorts were matched by propensity score without including colonoscopies, and the third set of cohorts were matched by propensity score with colonoscopies, colorectal adenomas, and appendectomies included. In the second set of cohorts, 36,864 persons with hemorrhoids that were diagnosed from 2000 to 2010 and a comparison cohort, with the same size and matched by propensity score, were established and followed up to the end of 2011 to assess the incidence and Cox proportional regression-measured hazard ratio (HR) of CRC. The overall incidence rate of CRC was 2.39 times greater in the hemorrhoid cohort than it was in the comparison cohort (1.29 vs. 0.54 per 1000 person-years), with a multivariable model measured adjusted HR of 2.18 (95% CI = 1.78–2.67) after controlling for sex, age, and comorbidity. Further analysis on the CRC incidence rates among colorectal sites revealed higher incidence rates at the rectum and sigmoid than at other sites, with adjusted HRs 2.20 (95% CI = 1.48–3.28) and 1.79 (95% CI = 1.06–3.02), respectively. The overall incidence rates of both cohorts were similar in the first and second sets of cohorts, whereas the rate was lower in the third set of hemorrhoid cohorts than in the respective comparison cohorts, probably because of overmatching. Our findings suggest that patients with hemorrhoids were at an elevated risk of developing CRC. Colonoscopy may be strongly suggested for identifying CRC among those with hemorrhoids, especially if they have received a positive fecal occult blood test result.

Piles in Pregnancy – Causes, Symptoms, Treatment & Health Tips
Hemorrhoids / Piles during pregnancy in younger women are not uncommon and can cause itching, discomfort and sometimes bleeding during bowel movement.

Round Table 142: Navigating ICD-10-CM Diagnosis Coding Hot Spots – Ciox
Coding Hot Spots Its accessible through a link that will provide in our follow-up e-mail, we sent out this afternoon.
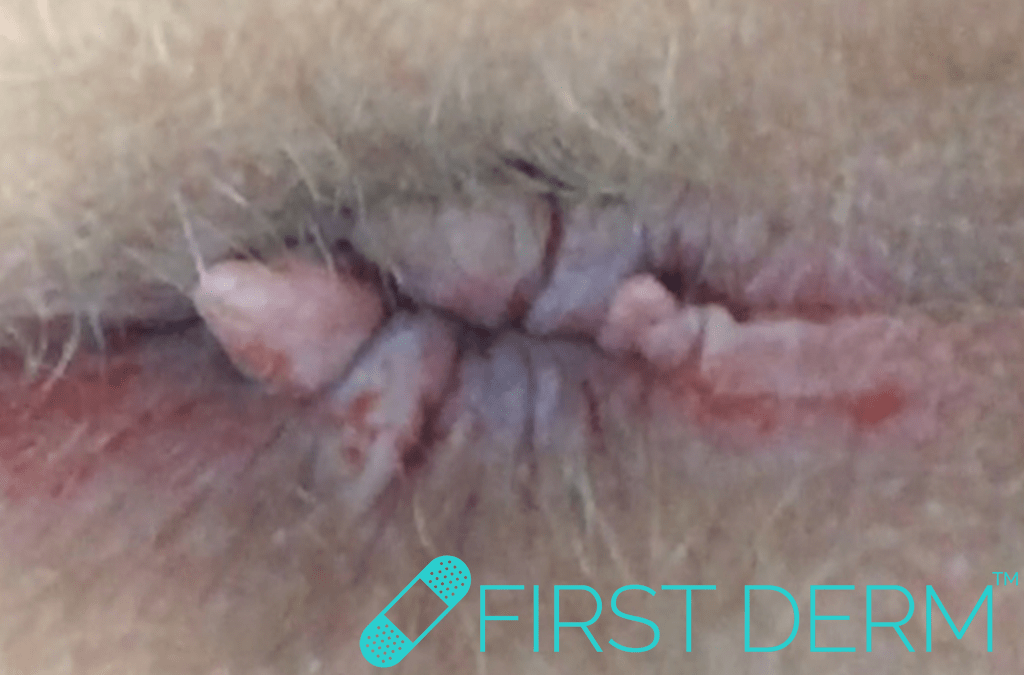
Hemorrhoids – Online Dermatology
Hemorrhoids are a normal part of the rectal area and is very common but harmless. They are the veins that encompass the mucus membranes in this region
![]()
Genome-wide analysis of 944,133 individuals provides insights into the etiology of hemorrhoidal disease | medRxiv
Hemorrhoidal disease (HEM) affects a large fraction of the population but its etiology including suspected genetic predisposition is poorly understood. We conducted a GWAS meta-analysis of 218,920 HEM patients and 725,213 controls of European ancestry, demonstrating modest heritability and genetic correlation with several other diseases from the gastrointestinal, neuroaffective and cardiovascular domains. HEM polygenic risk scores validated in 180,435 individuals from independent datasets allowed the identification of those at risk and correlated with younger age of onset and recurrent surgery. We identified 102 independent HEM risk loci harboring genes whose expression is enriched in blood vessels and gastrointestinal tissues, and in pathways associated with smooth muscles, epithelial and endothelial development and morphogenesis. Network transcriptomic analyses of affected tissue from HEM patients highlighted HEM gene co-expression modules that are relevant to the development and integrity of the musculoskeletal and epidermal systems, and the organization of the extracellular matrix. We conclude HEM has a genetic component that predisposes to smooth muscle, epithelial and connective tissue dysfunction. ### Competing Interest Statement The authors have declared no competing interest. ### Funding Statement This project was funded by Andre Frankes and Clemens Schafmayers DFG grant Discovery of risk factors for hemorrhoids (ID: FR 2821/19-1). The study received infrastructure support from the DFG Cluster of Excellence 2167 Precision Medicine in Chronic Inflammation (PMI) (DFG Grant: EXC2167). The project was supported by grants from the Swedish Research Council to MD (VR 2017-02403), the Novo Nordisk Foundation (grants NNF17OC0027594 and NNF14CC0001) and BigTempHealth (grant 5153-00002B). The work on cross-trait analysis for diverticular disease presented in this manuscript was supported by the German Research Council (DFG, ID: Ha3091/9-1) and the Austrian Science Fund (FWF, ID: I1542-B13). EGCUT work has also been supported by the European Regional Development Fund and grants SP1GI18045T, No. 2014-2020.4.01.15-0012 GENTRANSMED and 2014-2020.4.01.16-0125. This study was also funded by EU H2020 grant 692145 and Estonian Research Council Grant PUT1660. ### Author Declarations I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes The details of the IRB/oversight body that provided approval or exemption for the research described are given below: The enrolment of study participants was approved by the ethics committees or institutional review boards of all individual participating centers or countries. Written informed consent was obtained from all study participants. All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived. All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived. Yes I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance). Yes I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable. Yes The data supporting the findings described in this study are available from the corresponding author upon request.
Digestive Health Associates
Review of frequently asked questions relating to colonoscopy

Kode icd 10 hemorrhoid external, Interna, Grade 1, 2, 3, dan 4 – INOVASITEKNO.COM
Kode icd 10 hemorrhoid external, Interna, Grade 1, 2, 3, dan 4 – Hemoroid adalah penyakit yang ditandai dengan pembesaran pembuluh darah di daerah anus.
Consider How to Add Complication Visits To the Global Ob Package : Obstetrics
Hint: You can report complications before or after delivery. You can receive increased reimbursement when your ob-gyn provides additional visits outside of the normal global Ob package, but you’ll have to make sure you’ve coded high-risk or complicated obstetrical care correctly — and that means […]

VA Disability Ratings for Hemorrhoids – Hill & Ponton, P.A.
The VA rates hemorrhoids under 38 CFR § 4.114 Schedule of Ratings , with 0%, 10%, and 20% ratings being possible.

Hämorrhoiden | Gelbe Liste
Hämorrhoiden gehen oft mit analem Juckreiz, Schmerzen, Blutungen und Nässen einher. Im Stadium I und II kommen stuhlregulative Maßnahmen, Verödung und Gummibandligaturen zum Einsatz, in höheren Stadien (III–IV) ist meist eine operative Therapie erforderlich.
Hemorrhoids – Online Dermatology
Hemorrhoids are a normal part of the rectal area and is very common but harmless. They are the veins that encompass the mucus membranes in this region

Piles Types, Causes and Symptoms | Piles Laser Treatment in Hyderabad
Piles And Laser Surgery What Are Piles? Piles or hemorrhoids are the swollen and dilated blood vessels in the lower rectum and around the anus. In India, eve…

Hemorrhoidectomy | PDF | Hemorrhoid | Surgery
Hemorrhoidectomy – Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free.
10 tips to Get Rid of Haemorrhoids/Piles | Dr. Abhijit Gotkhinde
Are you suffering from painful hemorrhoids? Here are the 10 tips to Get Rid of Haemorrhoids/Piles by Dr. Abhijit Gotkhinde
Piles Types, Causes and Symptoms | Piles Laser Treatment in Hyderabad
Piles And Laser Surgery What Are Piles? Piles or hemorrhoids are the swollen and dilated blood vessels in the lower rectum and around the anus. In India, eve…
Hemorrhoidal disease: Diagnosis and management – Mayo Clinic
Rubber band ligation has been shown to be a safe, effective and painless therapy for grade I and grade II hemorrhoids. Although less durable than surgical excision, it is also less costly, has fewer complications and zero recovery time.